WA abortion researcher says executive order makes 'zero difference'

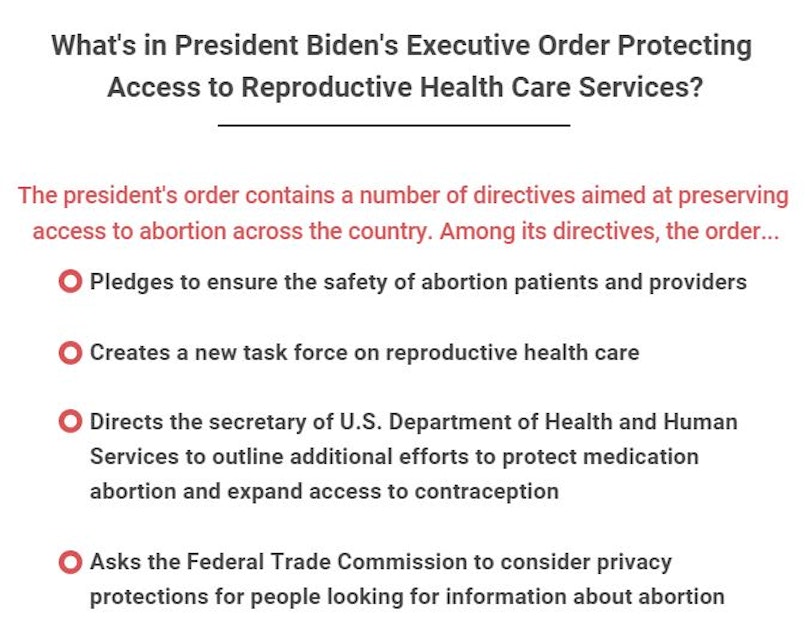
Many abortion rights advocates and providers are not satisfied with a recent executive order signed by President Joe Biden to safeguard abortion services across the country.
Even in states like Washington, providers liked Dr. Meghan Eagen-Torkko say the order is not enough to alleviate the fear some of her patients and colleagues feel now that the U.S. Supreme Court has overturned federal protections under Roe v. Wade.
"For me, the executive order makes zero difference, and I don't see it as being protective for my colleagues in other states," Eagen-Torkko said. "[And] I will say that, even in Washington state... my patients often are uncertain about what their options are for an unintended pregnancy."
Eagen-Torkko, an associate professor and director of nursing at the University of Washington Bothell School of Nursing and Health Studies, says Washington state lawmakers have done a lot to preserve access to abortion and protect those involved. But those efforts are still inhibited, to some degree, because people hear that Roe v. Wade was overturned and may not understand what that means for them. That uncertainty is leading more people to consider long-acting contraception, like intrauterine devices, or IUDs. Providers reported a similar uptick in IUD interest after former President Donald Trump was elected in 2016.
"People are asking for reliable contraception because they feel uncertain about whether or not they'd be able to access abortion if they needed it," Eagen-Torkko said. "I am absolutely supportive of people choosing implants and IUDs if it's the right method for them. But it needs to be a choice that they make and not, 'This is what I'm doing because I'm afraid that I'm not going to have another option.'"
Eagen-Torkko spoke with KUOW soon after the Supreme Court ruled struck down abortion protections, and she returned to explain why Biden's executive order does not alleviate her concerns.
This interview has been edited for clarity.
Angela King: We spoke to you right after the U.S. Supreme Court decision came down, and you said you had several concerns at that time, ranging from whether patients would be honest with their providers to fears over whether the decision would drive people out of the medical field. Does this executive order alleviate any of those concerns?
Sponsored
Dr. Meghan Eagen-Torkko: It doesn't. There are several problems with the executive order, the first of which, of course, is that it doesn't really have any teeth to it. The second is that what is legal is not always the extent of what is practiced, because fear for providers absolutely plays a role in what we can do.
You were also worried about how the Supreme Court ruling could interfere with doctor-patient relationships. We've already got a case involving a 10-year-old girl who was given a medication abortion, one where she took pills to end the pregnancy. That sparked a standoff between a doctor in Indiana and the attorney general of Ohio, where the girl was from. That case is unique for several reasons, but what was your reaction as a provider? Is that the sort of interference you are afraid of?
Yes. For me, my concern as a provider is that people are not going to be able to get the care that they need. And in this case, in Ohio, this patient was absolutely appropriately referred to a state where she could get the care that she needed — although, of course, she should have been able to get it in her home state. The problem is that now that provider is being scrutinized for the care that they provided, that was legal in Indiana. So, that is going to have an effect, going forward, for providers. It's not just about what's legal. It's not just about what, technically, you can do. It's about keeping your practice, keeping your admitting privileges and being able to continue this career that we love and that we have spent an enormous amount of time and energy developing the ability to do.
One of the things that was really striking about the Ohio case was actually how much blowback the reporters who were reporting on that story received. Essentially, there was the idea that there wasn't enough documentation for this to have been a real story. And one of the arguments was made that there was no police report, which, of course, ended up not being true. The reality is that the vast majority of sexual assaults in the U.S. are not reported to authorities for a number of reasons, not the least of which is that it can be doubly traumatizing, and that is particularly true for minors. So, if our standard of who gets to have an abortion is that a report is made in a timely fashion or that enough people know about it or that there are enough verifiable sources by some outsider's assessment, then what we're really talking about is that no one is going to be able to have an abortion because these things are very, very hard to document.
Sponsored
Well, as I mentioned at the top of our discussion, the executive order has been criticized for being vague. Do you think it addresses some of the specific health issues you raised, like how to treat miscarriages and ectopic pregnancies?
I think that it attempts to do so. I think that expecting it to make an actual difference in the care that is provided is unrealistic. One of the things that is addressed in the executive order is the idea that medication abortion cannot be banned and must be accessible because it's an FDA-approved medication. That is a lovely idea; the reality is what should be and what is are very, very different things.
When I was practicing in Michigan, in miscarriage management for cervical preparation for an IUD insertion, it was common practice at the time to prescribe misoprostol, which is one of the medications used in medication abortion. It was believed at the time that it improved the chances of success for the IUD insertion. So, I would write these prescriptions and write on them "this medication is to be taken for IUD insertion preparation" very clearly on the prescription in large letters. Yet my patients would have an extraordinarily difficult time filling those prescriptions. They were refused fills on this prescription by pharmacies who believed that they were being used for medication abortion. So, while I believe this executive order has the best of intentions — and probably is all that could be asked from the president at this time — it is not going to make a difference in terms of what people actually experience.
And of course, executive orders can be rescinded by the next administration.
Of course. That is always a concern. And in the case of abortion access in the United States, I don't believe that this one is going to have any real impact on whether or not people are able to access abortion care. I wish it did. I don't think it's going to.
Sponsored
Is there anything else you would like to add, doctor?
This is not going to be a short-term problem, and it's not going to be a short-term fix. We are at the start of another public health crisis. And I know that we're all very tired of public health crises because of the pandemic and because of everything else that's been going on. But this access to abortion care, this access to safe management of ectopic pregnancies and of miscarriages is going to be an ongoing crisis for us.
Health care, pregnancy emergencies and pregnancy complications are very rarely black and white. How close to death does someone have to be to qualify under a life exception in one of the states that have banned abortion except for life and health exceptions? How sick do you have to be? There's at least one health-care facility in another state that has told people that unless they're ectopic pregnancy is making them hemodynamically unstable, meaning that they are having internal bleeding, they cannot end their pregnancy. And we know that this is going to continue to happen because we have seen this before. What we don't know is what is going to be in place to keep people safe.
Sponsored
-
Katie Campbell

Online Editor/Reporter
Katie joined KUOW's online team as an editor and reporter in 2024, after serving three years as senior producer of the local Morning Edition program. She has covered a variety of local topics, including the Seattle City Council, elections, and breaking news. She also brings readers some levity with a weekly news quiz.
More stories from Katie Campbell » -
Angela King

Morning News Host
Angela King is the local host of Morning Edition. She’s been a part of the northwest news scene since the early 1990s. A proud University of Washington alumna, with degrees in broadcast journalism and American ethnic studies, she started her career as a news writer in Seattle, before becoming a reporter and anchor in Seattle, Portland and Albuquerque.
More stories from Angela King »


